In “Why does long COVID happen ?” we discussed the many contributing factors and interactions of processes that in some patients lead to chronic, ongoing issues affecting many aspects of health – and subsequently, daily lives. Dr. Bruce Patterson, formerly the Medical Director of Diagnostic Virology at Stanford University Hospitals and Clinics, California and now the founder of IncellDX, has with a team of clinicians designed a protocol that seeks to assess patient status through comprehensive lab analysis and then reduce the over-arching inflammation that can continue to cause symptoms. Dr. Patterson’s protocol has two main goals:
To explain a bit further, non-classical monocytes are capable of causing inflammation throughout the body in response to a chemokine called fractalkine/CX3CL1 (chemokines are important factors for cellular recruitment into inflamed tissues) and RANTES/CCR5. CX3CL1 is abundantly expressed by activated endothelium and is an important regulator of many aspects of endothelial function and dysfunction, including thrombosis. When upregulated, it is contributing to a pro-thrombotic environment and immune cell recruitment Chemokines are important factors for cellular recruitment into inflamed tissues RANTES is a chemokine that is stored in the alpha granules of platelets that can be rapidly released after platelet activation RANTES binds to the chemokine receptor CCR5. CCR5 is a chemotactic molecule that can amplify inflammatory responses and is expressed on immune cells such as T-lymphocytes, macrophages, and NK cells. CCL5/RANTES acts like a magnet for these immune cells expressing CCR5. CCL5/RANTES is a marker for the early stages of immune dysregulation in COVID-19 and as a possible therapeutic marker to determine when and how long therapy targeting CCR5 or RANTES should be continued. The Protocol Important reminder: this protocol should be utilized ONLY by those clinicians who understand the mechanisms behind long-haulers syndrome and who have experience treating this complex patient group. The treatment protocol is usually given for four to six weeks, with the goal to restore immune balance. A follow-up visit is then to done to assess response to the protocol; note that some patients may need longer courses of therapy dependent upon variable factors including their individual health issues and/or response to treatment. With Dr. Patterson’s protocol, a specialized series of labs, the IncellKINE test, are conducted (note: the Incell DX panel should be used only as guidance of treatment). Based on those results, patients are then typically prescribed these therapies below; but, every patient is different and unique so each protocol is specific for each patient. Many times we repeat the Incell DX panel to gauge treatment response and follow clinical response as well. A. Maraviroc A CCR5 antagonist, Maraviroc reduces cytokines and blocks migration of the intermediate and non-classical monocytes and repolarizes the macrophages and modulates the immune system. We know that CCL5/RANTES is commonly elevated in long COVID and as an antiretroviral, Maraviroc also has been used in combination with other drugs to treat diseases including human immunodeficiency virus (HIV).
Possible side effects Orthostatic hypotension One case of hepatotoxicity Black box warning for liver toxicity so liver function tests and complete blood counts should be checked monthly while undergoing treatment with Maraviroc. B. Statins to tamp down the CX3CR1/fractalkine pathway In order to turn off the long-term monocyte survival mechanism that’s allowing these cells to endure longer than usual. As such, statins are the second prescribed drug in the protocol. They work by inhibiting fractalkine, which stops the monocyte cells from attaching to endothelial cells on the blood vessels.
C. Ivermectin As an immunomodulator and anti-parasitic drug prescribed because of its immunomodulating effects, ivermectin is the third prescribed medication in Dr. Patterson’s protocol. It is thought to help detach and then bind to the spike protein, thereby rendering it incapable of attaching to the cell membrane. The ivermectin docking to ACE2 receptors may interfere with the attachment of the spike to the human cell membrane; it has been shown to inhibit lipopolysaccharide (LPS) induced, proinflammatory cytokines and improve survival in mice. Note that LPS is an endotoxin that can cause systemic inflammation. Ivermectin lowers these cytokines: ↓TNF--α ↓IL-1ss ↓IL-4 ↓IL-5 ↓IL-6 ↓IL-13 Recommended dosage is .2-.4mg/kg each day, for 3-5 times a week (note that higher and/or longer dosing are sometimes needed). After 3-5 days, reduce dosing schedule to 1-2 times/week then discontinue after 2-4 weeks. D. Mast cell stabilization It all has been suggested that mast cell activation can play an important role in long COVID or post-acute sequelae of COVID-19 (PASC) due to atypical responses to SARS-CoV-2 by the dysfunctional mast cells. Therefore, stabilizing mast cell activity can be a critical effort in treating long COVID patients. The Front Line COVID-19 Critical Care Alliance (FLCCC) offers a protocol of care to address mast cell activation, as noted in the following chart: 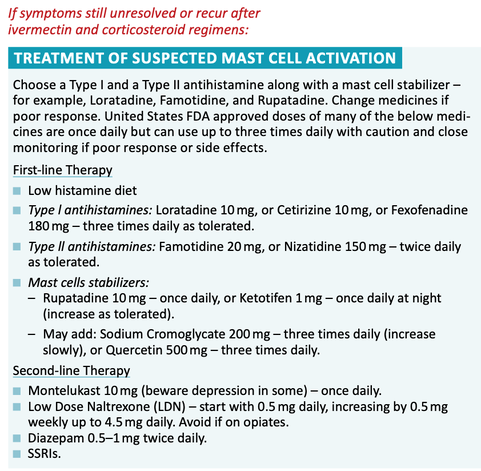 Other ways to address mast cell activation
E. Monocyte repolarization from M1 to M2
F. Fluvoxamine: Brand name Luvox, this long-available serotonin-reuptake inhibitor has been typically used for treating depression. The protocol here recommends 25-50-100 mg twice daily, (can substitute 20- 30mg Prozac QD) to activate sigma-1 receptors decreasing cytokine production. Fluvoxamine has been found to have positive effects on autophagy and SSRI inhibition of platelet activation. G. Prednisone Many Long Hauler protocols will utilize short courses of steroids. Sometimes even a low dose of 5 mg per day can be helpful; higher doses may be necessary as well dependent upon patient status and tolerance. A tapering dose of prednisone of .5 mg/kg for 5 days; .25 mg/kg for 5 days; followed by .12mg/kg for an additional 5 days. Patients should take in the morning to lessen impact on sleep. In some cases, a steroid-sparing agent such as methotrexate, dosage 7.5 mg/week, along with folic acid supplementation may be helpful. H. IVIG In some patients, intravenous immunoglobulin (IVIG) treatment can be helpful in recovery. IVIG has been demonstrated to:
I. LDN (immunomodulation) Low Dose Naltrexone .5-4.5 mg / day The opioid antagonist naltrexone hydrochloride has been suggested to be a potential therapy at low dosage for multiple inflammatory conditions and cancers.
https://pubmed.ncbi.nlm.nih.gov/28536359/ Dr. Patterson’s protocol and his team’s work has done much to better understand the mechanisms involved in long COVID so the medical community subsequently can provide the most effective treatments. Coming soon! Given the complexity of issues that we are seeing occur every day and that vary from one patient to another, Dr. Robin Rose and I are creating a comprehensive integrative medicine program to help long haulers. Dr. Rose is known for her work in the field of internal medicine and gastroenterology that targets the human gut microbiome and understanding its link to health and disease. Our protocol and upcoming discussion will cover in more detail a number of other therapeutic measures including, but not limited to:
It’s important to keep in mind that as new information arises, so may some of the recommendations for therapies change with the evolution of this novel disorder. And as always, if you are experiencing any issues or symptoms that haven’t resolved with initial care, please don’t hesitate to consult your physician for guidance or feel free to reach out to our offices. We are here to help! In health and hope, Dr. Suzanne Gazda References: Sayana S, Khanlou H. Maraviroc: a new CCR5 antagonist. Expert Rev Anti Infect Ther. 2009;7(1):9-19. doi:10.1586/14787210.7.1.9 Lehrer S, Rheinstein PH. Ivermectin Docks to the SARS-CoV-2 Spike Receptor-binding Domain Attached to ACE2. In Vivo. 2020;34(5):3023-3026. doi:10.21873/invivo.12134 Zhang X, Song Y, Ci X, et al. Ivermectin inhibits LPS-induced production of inflammatory cytokines and improves LPS-induced survival in mice. Inflamm Res. 2008;57(11):524-529. doi:10.1007/s00011-008-8007-8 Lawrence B. Afrin, Leonard B. Weinstock, Gerhard J. Molderings. Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. International Journal of Infectious Diseases. November 2020. Glebov, Oleg O. Low-Dose Fluvoxamine Modulates Endocytic Trafficking of SARS-CoV-2 Spike Protein: A Potential Mechanism for Anti-COVID-19 Protection by Antidepressants. Frontiers in Pharmacology. 2021. https://www.frontiersin.org/article/10.3389/fphar.2021.787261 DOI 10.3389/fphar.2021.787261 Gazda Integrative Neurology https://www.suzannegazdamd.com/blog/more-reasons-for-more-vitamin-d incellDX https://incelldx.com/ Saha C, Kothapalli P, Patil V, ManjunathaReddy GB, Kaveri SV, Bayry J. Intravenous immunoglobulin suppresses the polarization of both classically and alternatively activated macrophages. Hum Vaccin Immunother. 2020;16(2):233-239. doi:10.1080/21645515.2019.1602434 Das, M., Karnam, A., Stephen-Victor, E. et al. Intravenous immunoglobulin mediates anti-inflammatory effects in peripheral blood mononuclear cells by inducing autophagy. Cell Death Dis 11, 50 (2020). https://doi.org/10.1038/s41419-020-2249-y
8 Comments
Heather Rae
8/1/2022 05:23:58 pm
There is no evidence of SARS CoV2 in a human being, and no legitimate test for spike protein in a human being.
Kenneth Phillips
12/17/2022 11:09:29 am
I supposed that you are going to tell me that the 6,667,509 people that have died from COVID really aren't dead.
Mark
1/3/2023 11:00:02 am
You’re misinformed . Covid 19 is a very real bio weapon. The longer you deny this the more people you prevent from finding out the truth so they can start healing
Paul Elkins
8/3/2022 10:18:46 am
Thanks so much for providing a comprehensive review of the most promising treatments for PASC! I also very much appreciated your review of the various MOAs and support for each therapeutic. There are so many suffering with PASC and being left on their own, told their symptoms are all psychological, and denied any support.
Kenneth Phillips
12/17/2022 10:04:25 am
Great review of some of the things that have helped me personally on the road to recovery from long COVID starting two years ago.
Kenneth Phillips
12/17/2022 11:08:10 am
The only other thing that was helpful not mentioned here is Nattokinase/Serrapeptase
Mark
1/3/2023 10:58:21 am
Hello and thank you for this resource! I’ve been taking ivermectin for the past five days prescribed by my doc. I’ve also been taking quercitin and bromelian supplements. I’m definitely improving but not fully back to normal yet. But this morning I read there is a possible interaction between quercitin and ivermectin that could inhibit effectiveness of ivermectin? should I be concerned about this? Help. Thanks
Stacy Weller
2/22/2023 07:37:35 am
How do I find someone in my state using this protocol? Your comment will be posted after it is approved.
Leave a Reply. |
AuthorSuzanne Gazda M.D. Neurologist Archives
January 2024
Categories |
 RSS Feed
RSS Feed